Herd Immunity occurs when enough persons either have had a disease and recovered (so that they can’t get the disease again), or have received a vaccine. When the Herd Immunity Threshold (HIT), a certain percentage of the population, can no longer catch a disease, they can no longer be part of the spread of the disease. At that point, HIT, so many persons are immune to the disease that the number of new cases continually drops, until it reaches zero. Therefore, reaching Herd Immunity is a way to end the Covid-19 pandemic. In fact, the purpose of the current Covid-19 vaccination program is to reach HIT, so that the spread of the pandemic will decrease and finally end.
The R-nought value (R0) is a measure of how quickly a disease spreads. It is the number of persons, on average, who catch the disease, from each infected person. If each person with Covid-19, on average, infects 2.5 other persons, then the R0 for Covid-19 is 2.5. The Herd Immunity Threshold is based on R0. The slower a disease spreads, the lower the HIT (% of population who need to be immune to stop the pandemic).
Now here is the point of this article: Anything we can do to lower the R0, and thereby lowers the number of persons who need to be vaccinated to reach HIT and end the pandemic. Which interventions lower R0? Vitamin D, some other supplements, and the medication Ivermectin. First and foremost, Vitamin D greatly reduces risk from Covid-19. A massive immediate population-wide vitamin D supplementation program will lower the R-nought value (i.e. lower the spread of Covid-19). This lowers the HIT value, meaning that far fewer persons will need to be vaccinated to reach Herd Immunity. And once we reach Herd Immunity, the pandemic slows to a stop.
Examples of Herd Immunity
Hypothetical example: 100 persons in a city have a disease, they each pass on the disease, on average, to 3 persons. This number is called the R-nought (R0) value: average number of persons who catch a disease from each infected person. So in this hypothetical, the R0 is 3. Therefore, in the next “generation” of the disease, 300 more persons become ill (100 x 3). And next 900 more persons become ill (3 times 300), and so on. That is how a disease spreads and becomes a pandemic. But with Herd Immunity, most of the persons who would have become sick were already immune. So the first 100 persons only pass on the disease to an average of less than 1, which means, say, 80 persons catch the disease from that group of 100. So the second generation is 80, instead of 300 (because 220 out of 300, about 73%, were immune), and the third generation is 64 instead of 900, and so on. Quickly, the disease dies out.
Real Life Example: Measles is highly contagious. It has an R-nought or “R0” value of 18. That means each person who gets measles will, on average, spread it to 18 other persons. Eighteen!! But if almost everyone has been vaccinated against measles, then a person who gets measles cannot spread it to 18 persons, as in almost all cases the 18 persons who would have caught the disease are already immune.
What percentage of persons needs to be vaccinated against measles to prevent its spread by herd immunity? The formula begins by finding one divided by the R0 value (1/R0), then subtract that from one and the result is the percentage of the population that must be immune to prevent the spread (or to stop a pandemic)
1 - 1/R0 = Herd Immunity Threshold (HIT value)
For measles, that HIT value is 94.44%, which is the percent of the population who must be immune to stop the spread of the disease. They can be immune either because they had the disease and recovered, or because they have been vaccinated.
Covid-19 Herd Immunity
The CDC estimates the R0 value of Covid-19 to be 2.5 [Explanation at CDC.gov].
1 - 1/2.5 = 60% of the population
If we had a vaccine against Covid that was 100% effective, then 60% of the population would need to be vaccinated. If the vaccine is 94% effective, then the percentage vaccinated, times 0.94, must equal that 60%. In this example, ~63.8% of the population would need to be vaccinated with a 94% effective vaccine to protect 60% of the population and thereby reach Herd Immunity. So with a population of 330 million in the U.S., 60% is 198 million persons. Since the vaccine is only 94% effective, 63.8% of the population, which is ~211 million persons, would need to be vaccinated for 198 million to be immune (rounding up to nearest million).
However, some persons are immune to Covid-19 because they had the disease and recovered. So the number who need to be vaccinated to reach 198 million immune persons is lower, since it includes those who recovered from Covid-19 (and so obtained immunity in that way). How many persons have recovered fully from Covid-19 and therefore are already immune in that manner?
According to Worldometers, about 11.7 million person have recovered from Covid-19 in the U.S. However, many persons who became ill with Covid-19 do not see a doctor, and simply remain at home. The actual number who are immune from recovery from Covid may be much higher. But let’s be conservative and estimate that about the same number go unreported as reported. That gives us about 24 million persons in the U.S. who are immune by recovery from Covid. Some of those might be able to get the disease again, just as some vaccinated persons might be able to get Covid despite the vaccine.
Note that 24 million persons is ~7.3% of the U.S. population. So let’s subtract the 7.3% from the 63.8% and only 56.5% or 186.5 million need to be vaccinated with an R-nought value of 2.5.
Once we vaccinate 186.5 million persons, which is 56.5% of the U.S. Population, we will reach Herd Immunity Threshold (HIT). The problem is that we would have to vaccinate more than a million persons a day to reach HIT soon enough to avoid catastrophic failure of our healthcare system and our economy. We cannot vaccinate fast enough at this point in time!
Solution: Lower the HIT value, i.e. lower the percent of the population who need to be vaccinated by lowering the R-nought value via Vitamin D and other supplements, along with Ivermectin for high-risk persons. Here is a chart of (A) the R0 value and (B) the corresponding HIT value and (C) number of persons needing vaccination to reach Herd Immunity. The HIT = 1 - (1/R0). But C is calculated taking into account recovered cases: C = ((HIT%/94%) - 7.3%) times 330 million (total U.S. pop.)
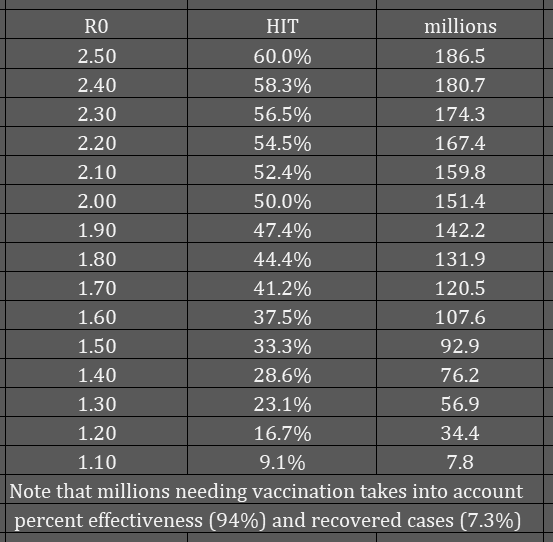
If we could reduce the R0 value to 2, so that each infected person only transmits the disease to two persons on average, we can reduce the HIT to 50% of the population who need to be immune. But the vaccine is only 94% effective, raising the percent to 53.2. But 7.3% are already immune, having recovered from a case of Covid-19, which lowers it to 45.9% of the population who need to be vaccinated, which is about 151 million persons. That reduces the number needing vaccination by about 35 million persons.
If we could lower the R0 value to 1.5, so that each set of 100 infected persons only transmits the disease to, on average, 50 persons (1 transmission per 2 infected), then the number who need to be vaccinated is about 92.9 million persons, or about 28% of the population. Note that the HIT column is the percent who need to be immune, but the millions needing vaccination takes into account that the vaccine is not 100% effective (it is 94% effective) and that 7.3% are already immune by recovering from a case of Covid-19.
** Which is the better goal for number to be vaccinated, 186.5 million, or 151 million, or 92.9 million? We can reduce the number of persons who need to be vaccinated IN HALF by reducing the R0 value to 1.5 from its current 2.5. Reducing to 2.0 still leaves us with too many persons needing vaccination (151 million). We can vaccinate 93 million persons in 3 months at 1 million a day. And that is the slowest rate of vaccination that is tenable.
HOW DO WE GET FROM THE CURRENT R0 VALUE OF 2.5 DOWN TO 1.5? We must reduce the R0 value to no more than 1.5, so that the number needing vaccination is no more than 93 million (3 months). We cannot vaccinate 186.5 million persons in less than 6 months. To cut the time to Herd Immunity in half, 3 months instead of 6 months, we must lower R0 to 1.5.
The current R0 of 2.5 already takes into account using masks and social distancing, and going out less often. We need something more that we can do to lower the R-nought value.
The Vitamin D Solution
The supplement with the strongest evidence for a reduction in risk of contracting Covid-19 (thereby reducing the R0 value) is vitamin D. Over fifty studies of Covid-19 and vitamin D have found that normal blood levels of vitamin D greatly reduce risks from Covid-19, including risk of infection, risk of a severe case, risk of needing hospitalization, risk of needing ICU care, risk of needing oxygen and/or mechanical ventilation, and risk of death from Covid-19. See this linked page for all the studies.
So in addition to reducing the R-nought value with vitamin D supplementation, we would also be reducing the percentage of cases that are severe, reducing the percentage of cases that need hospitalization, and reducing the need for ICU, ventilation, and other medical resources, and reducing the percentage of Covid-19 patients who die.
It is well-proven [2] that blood levels of vitamin D in the general population in the U.S. fall in winter, and rise in summer. This explains why there has been a Winter Wave of Covid-19 cases. Covid-19 is highly responsive to vitamin D. In the U.S., October had about 2 million cases of Covid-19, November had about 4.5 million, December will have just over 6 million cases, but about twice as many deaths as Nov. Why are deaths increasing in December faster than cases are increasing? It is because hospitals are absolutely full and are turning away patients they would have admitted a month ago. They don’t have the beds or the staff. So the number of reported cases, always lower than actual number of cases, is now much lower than actual cases, as the hospitals are full.
January, February, and March will absolutely break the hospital system. And the vaccination program will NOT be able to vaccinate enough persons in time. Also, the current vaccines require a shot, a waiting period of 3 or 4 weeks, another shot, and then full protection does not kick-in until a week or two after that second shot, respectively (Pfizer, Moderna). And we can only vaccinate so many persons per month. The vaccine program will NOT save the hospital system from collapse. But vitamin D can reduce risk of Covid-19 in so many ways, to such an extent, as to reduce cases, hospitalizations, and deaths. And a bolus dose of vitamin D is the safest and fastest way to raise blood levels to normal range [3].
Vitamin D reduces risk of contracting Covid-19 by more than 50%. The Kaufman study [1] found that those with low levels of vitamin D were much more likely to test positive for Covid-19 than persons with higher blood levels. Persons with a vitamin D level of about 50 ng/ml had about half the risk of infection of persons with a vitamin D level just under 20 ng/ml. See also this article: Vitamin D can help reduce coronavirus risk by 54%: Boston University doctor.
In the U.S. in winter, about half the population has vitamin D deficiency and about another one quarter of the population has vitamin D insufficiency [2]. What would happen to the Covid-19 pandemic if we raised their levels of vitamin D to normal range? This can be accomplished in a matter of days or weeks, once the person begins taking vitamin D. If everyone had normal vitamin D levels, the risk of contracting Covid-19 would be reduced severely. In the Katz study, “patients with vitamin D deficiency were 5 times more likely to be infected with Covid-19 than patients with no deficiency” [4]. Most of the cases of Covid-19 are found in the population that is vitamin D deficient or insufficient.
Raising the vitamin D levels of any population — a family, a workplace, a nursing home, the medical staff at a hospital, a town, city, state, province, or nation — reduces the number of Covid-19 cases, hospitalizations, and deaths. This also lowers the R-nought value, thereby lowering the Herd Immunity Threshold, bringing an end to the pandemic nearer. A widespread vitamin D supplementation program will reduce the number of persons who need vaccination from 186.5 million to about 93 million.
How Much Vitamin D?
Over 120 physicians, researchers and other experts signed the Vitamin D for All letter here. (I know it says over 100, but dozens more have signed since it first came out.) This Letter recommends Vitamin D3 at 10,000 IU per day for 3 weeks, and then 4,000 IU per day thereafter.
For those who are ill with Covid-19, studies have shown that a high dose of vitamin D for several days reduces days to recovery. There are multiple studies, see the list of over 50 studies here. Those who have Covid-19 should take 100,000 IU of vitamin D3 per day for 5 days. Studies of large doses of vitamin D3 have found that a dose of 500,000 IU is safe and effective at quickly raising vitamin D blood levels [3]. After the 5 days, take the usual 4,000 IU of vitamin D3 per day continuously.
Ivermectin
Persons who are at high risk of contracting Covid-19, especially those who are also at high risk of a severe or fatal case, should take the vitamin D, but the should also take ivermectin. The i-MASK protocol suggests the use of ivermectin as a prophylactic against Covid-19. There are enough studies to prove that ivermectin is both safe and effective. See the Ivermectin studies and information here.
The i-MASK protocol recommends ivermectin for those at high risk of Covid-19. The dosing is 0.2 mg of ivermectin per kg of body weight. This works out to 0.09 mg per pound of body weight.
Examples:
Your weight times 0.09 mg equals mg per dose of ivermectin
100 lbs = 9 mg of ivermectin
150 lbs = 13.5 mg
200 lbs = 18 mg
You do not need to take exactly 0.2 mg per kg of body weight (0.09 mg per pound of body weight). Round the number to the nearest 3 mg. There is a body weight to dosage conversion chart on this page.
Once you have calculated the right dose, take that dose as follows:
First dose (day 1)
Skip a day (day 2)
Second dose (day 3)
For treatment of Covid-19, that is all you take, two doses separated by one day without a dose. For prophylaxis (prevention), you take the two doses the first week, and then one dose only, every other week.
The i-MASK protocol also suggests Vitamin D, Vitamin C, Zinc, Quercetin, and Melatonin as part of their prophylactic program. Some studies have also found that selenium (200 micrograms per day) is effective in reducing risk of contracting Covid-19.
Vitamin D, Ivermectin, Vaccination
A vitamin D supplementation program will reduce the R-nought value, thereby reducing the Herd Immunity Threshold, thereby requiring fewer persons to be vaccinated to end the pandemic. This program, combined with vitamin D plus ivermectin for the highest-risk persons, should be able to reduce the spread of Covid-19 to an R0 value of 1.5. So every two persons who are ill would spread the disease to only one person.
Then the vaccination program should focus on those persons who are most likely to spread the disease, if they become sick. In this way, the R0 value will fall faster, as the vaccination program continues. Not everyone spreads the disease at the average of 2.5 transmissions per case. Vaccinating those who are most likely to spread Covid-19 to others — first responders, grocery store workers, restaurant and food workers, essential businesses — will also lower the R0 value, continually decreasing the number who need to be vaccinated.
The vitamin D program is paramount. It must begin immediately. It is not sufficient to leave it up to the public and merely give them a recommendation. Vitamin D should be distributed with the vaccine. Vitamin D should be distributed in institutions: schools, nursing homes, prisons, group homes, businesses, hospitals and clinics, etc. And vitamin D should be put into foods. Sweden has a substantial vitamin D food fortification program, which explains why Sweden was not hit as hard by the pandemic as many other European nations.
Vitamin D for everyone.
Ronald L. Conte Jr.
Covid.us.org
“an author, not a doctor”
1. Kaufman HW, et al. “SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels.” (2020) PLoS ONE 15(9): e0239252. Study Link
2. Kroll, Martin H., et al. “Temporal relationship between vitamin D status and parathyroid hormone in the United States.” PloS one 10.3 (2015): e0118108. Study Link
3. Kearns, Malcolm, Jessica Alvarez, and Vin Tangpricha. “Large, single-dose, oral vitamin D supplementation in adult populations: a systematic review.” Endocrine Practice 20.4 (2014): 341-351. Study Link
4. Katz, Joseph, Sijia Yue, and Wei Xue. “Increased risk for Covid-19 in patients with Vitamin D deficiency.” Nutrition (2020): 111106. Study Link

You are assuming that recovery leaves the recovered with immunity. This is proving not to be universally the case. Nor do we know how long any immunity will last.
LikeLike
It’s not universal, but it is common that the recovered have antibodies.
LikeLike