22 August 2020
Kaplin, Adam Ian, et al. “Evidence and magnitude of seasonality in SARS-CoV-2 transmission: Penny wise, pandemic foolish?.” medRxiv (2020). Submitted to PLOS ONE (under review). Study Link
14 August 2020
The entire world has had over 21 million reported cases of Covid-19 and over 750,000 deaths. This Winter, if Covid-19 is Seasonal, the United States alone could see that many cases and that many deaths, due to lower levels of vitamin D in the population.
11 August 2020
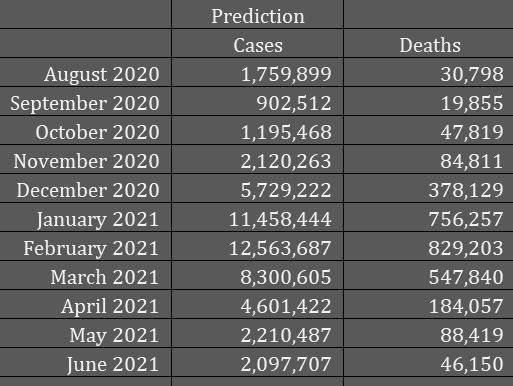
* Using the first 10 days from August, I’ve predicted 1,759,899 new cases for the whole month of August, with 30,798 deaths that month. Unfortunately, this suggests that the case rate and death rate this winter will be HIGH:
8 August 2020
The difference in deaths this winter from Covid-19 being seasonal, to not seasonal, is millions of lives in the U.S. alone, and tens of millions worldwide. The reason for the seasonality is not mainly weather, temperature, humidity, rainfall, or other factors. Rather, the reason for the seasonality of Covid-19 is the seasonal rise and fall in vitamin D levels in populations who live in climates that influence persons to spend much more time indoors than outdoors during certain months.
As vitamin D is not found in high concentrations in most foods, the majority of the vitamin D in the blood of human persons is from sunshine on skin. And this implies that spending more time outdoors, particularly while wearing less clothing, will result in higher vitamin D blood levels, whereas covering most of the body and/or remaining indoors, results in lower levels. With low levels of vitamin D comes lower resistance to contagious diseases, as vitamin D has an important role in the immune system.
Covid-19 is seasonal due to the rise and fall of vitamin D levels. Low vitamin D in winter means higher rates of infection, higher rates of severe and critical cases, higher rates of ICU admission, higher rates of mechanical ventilation, and higher rates of death. This winter — unless we undertake a massive vitamin D supplementation program — we will be overwhelmed with a vast number of cases and deaths, and the healthcare system will break.
It takes a month or two to raise vitamin blood levels by supplementation or sunshine. So we need to start as soon as possible.
7 August 2020
* What will the World’s cases and deaths from Covid be like this winter? July cases worldwide: 7,175,074 and July deaths worldwide: 169,206. In any peak winter month (Jan., Feb., March), deaths could be 5 to 10 times July, which is 35 to 70 million new cases in that month alone, and deaths would be anywhere from 2 million to 7 million. These figures are per month worldwide. Some nations will have higher percentages, and some will have lower percentages.
* Vitamin D supplementation and a “sunshine on skin” public service announcement program are the only way to avert this massacre, this second wave of cases and deaths.
6 August 2020
* Is Covid-19 Seasonal? Yes, it is. There are at least 18 studies showing that vitamin D blood levels have a substantial effect on the disease, higher levels are better; insufficiency or deficiency is worse, much worse. And we know that Vitamin D levels rise and fall from summer to winter. Furthermore, the other human coronaviruses, the ones that cause colds, are seasonal, very seasonal with many more cases in winter than summer/early fall.
This implies that the monthly cases we will see this coming winter will be a multiple of the cases we saw in July (2 million then). But the U.S. healthcare system cannot handle a multiple of 2 million cases in one month. So we must act. See below.
* Covid-19 is seasonal, and that means this winter the total cases per month will be a multiple of July. July was just under 2.0 million cases. February could be several times that number. The exact numbers don’t matter, as any multiple of 2 million cases per month is more than the healthcare system can handle. So I’m developing a plan. This is the working plan, that will develop and change in real time on this site.
A. “Sunshine on skin” program to convince persons in developing nations, who can’t afford supplements or medications, who don’t have any healthcare at all, who don’t even have water and soap for handwashing, to set aside religious and social customs, and get out in the sun. This will raise blood levels of vitamin D, protecting them from Covid-19.
“Despite an abundance of sunshine, studies from the Middle East show that there is a high prevalence of vitamin D deficiency in women of childbearing age, mainly attributed to cultural avoidance of sunlight and traditional dress style that cover most of the body while outdoors, and inadequate vitamin D intake.” [Dawodu, “Maternal Vitamin D Status: Effect on Milk Vitamin D Content and Vitamin D Status of Breastfeeding Infants” Adv. Nutr. 3: 353–361, 2012; doi:10.3945/an.111.000950]
B. Vitamin D supplementation. For developing nations and anyone who can afford it, high vitamin D supplementation:
Infants: 400 IU/day
Children, 1-3: 2,000 IU/day
Children, 4-8: 3,000 IU/day
Children, 9-13: 4,000 IU/day
Teens, 14-18: 4,000 IU/day
Adults, 19-59: 10,000 IU/day
Seniors, 60+: 20,000 IU/day
The children’s levels vitamin D supplementation above are derived from body weight charts (lower dose for lower weights). The infant dose is just the U.S. RDA (actually called “adequate intake” for infants).
C. Other supplements and OTC medications. For now, use the MATH+ recommendations on this page
D. Standardization of treatment protocols based on hospitals with the lowest death rates. Start with MATH+ and improve, then standardize. Give doctors options only within a certain range of treatments and medications.
E. Rapid building of multiple hospitals in 45 days as Turkey did news report here and also here.
F. After the pandemic is over, there will be a vast number of “survivors” of Covid-19 who have chronic damage from the disease. They will need extra medical care for the rest of their lives. This will weigh on the health care system. We need to plant for their care as follows:
(1) More medical schools and nursing schools, and more seats in each school,
(2) More training for medical technical positions,
(3) More hospitals, esp. tertiary care hospitals,
(4) a new type of hospital, dedicated solely to long-term treatment for chronic ailments, including “Covid-19 Survivors Syndrome” as well as cancer, organ transplants, veterans injured in war, etc.
(5) A nationwide very strong focus on prevention of diseases, like cancer and heart disease. Prevention is the only way to have enough resources to treat everyone. Healthcare for all is prohibitively expensive unless we prevent most illnesses. 90% of all cancer and heart disease and type 2 diabetes cases are preventable. Research on prevention must be followed up with implementation of research conclusions.
5 August 2020
* I’ve just started this page, which will remain at the top of the list of posts. My study of Covid-19 has reached the point where I need to spend more time, daily, explaining what all the research means, how it all fits together, and what we all must do to save millions of lives: main problems, proposed solutions, what will happen if we fail, etc.
Please read the article “If Covid-19 is seasonal…” This insight is crucial. If correct, it means we are headed towards a massive second wave of Covid cases, ramping up from October to November to the top of the wave: December, January, February and March.
Most estimates right now are saying that the monthly case totals will fall in October and November. They will not fall. Not unless there is a vitamin D “supplementation and sunshine program”. Instead, case numbers will rise in those months. And by December, the hospitals will be at the breaking point.
The number of dead from Covid-19 in this winter alone, in the U.S., will easily exceed half a million, and could be as high as 3 to 4 million. Those are just Covid-19 deaths, just from October to March.
Why? because Covid-19 is seasonal, and seasonal coronaviruses are worst in those months.
Consider supporting Covid.us.org with a one-time or recurring donation via PayPal
